Seat too far forward?

birdy247
Posts: 454
If my seat is too far forward would i use different muscles than if my seat was in the correct position or even too far back.
Particularly thinking about my calves, hamstrings and quads.
Particularly thinking about my calves, hamstrings and quads.
0
Comments
-
(Assuming your hip-to-pedal distance has remained constant) having your saddle forward, thus increasing your hip extension angle, results in lower hamstring, glute (and possibly calf too) and greater quad work, as far as I can remember. This is a relatively hot topic, because triathletes care about it - the push for steeper seat angles is partly aerodynamic, but partly to smooth the transition between cycle and run legs.0
-
Your saddle being too low or high is probably more important. If it feels comfortable stick with it, but if you feel a certain part of your leg or muscle is taking particular strain you might what to adjust it."A cyclist has nothing to lose but his chain"
PTP Runner Up 20150 -
If you seat is too far forward, you can suffer from pain behind the knee.0
-
0
-
sampras38 wrote:sandbag wrote:If you seat is too far forward, you can suffer from pain behind the knee.
I think if you mean if the seat is too high.
That's more likely to cause pain behind the knee.
Google it..;-)
A seat too far forward or back can have an affect on knee pain as can having your seat too high or too low. Seat too far forward can lead to pain in the front of the knee and pain at the back of the knee from seat too far back.0 -
doyler78 wrote:sampras38 wrote:sandbag wrote:If you seat is too far forward, you can suffer from pain behind the knee.
I think if you mean if the seat is too high.
That's more likely to cause pain behind the knee.
Google it..;-)
A seat too far forward or back can have an affect on knee pain as can having your seat too high or too low. Seat too far forward can lead to pain in the front of the knee and pain at the back of the knee from seat too far back.
Ah, thanks, I stand corrected. It was just a friend of mine was suffering from pain behind the knee, had a professinoal bike fit and they basically just ended up lowering his saddle. Fixed the problem straight away. Subsequently I've seen a lot of info on the web about a high saddle and pain at the back of the knee.
thanks though0 -
sampras38 wrote:sandbag wrote:If you seat is too far forward, you can suffer from pain behind the knee.
I think if you mean if the seat is too high.
That's more likely to cause pain behind the knee.
Google it..;-)
Yes that is the obvious case - too high saddle causes it, due to the leg been stretched out too much. Putting stress on tendons. Lots of contiuned cycling makes it worse. Complete rest is best to heal it.
I did look into it and also too far seat forward can also cause it, due to the position of the knee too far forward. The pressure is on the back of the knee more. As the OP was just asking about 'forward and aft positions', i didn't mention too high seat position.0 -
sandbag wrote:sampras38 wrote:sandbag wrote:If you seat is too far forward, you can suffer from pain behind the knee.
I think if you mean if the seat is too high.
That's more likely to cause pain behind the knee.
Google it..;-)
Yes that is the obvious case - too high saddle causes it, due to the leg been stretched out too much. Putting stress on tendons. Lots of contiuned cycling makes it worse. Complete rest is best to heal it.
I did look into it and also too far seat forward can also cause it, due to the position of the knee too far forward. As the OP was just asking about 'forward and aft positions', i didn't mention too high seat position.
No probs..;-)0 -
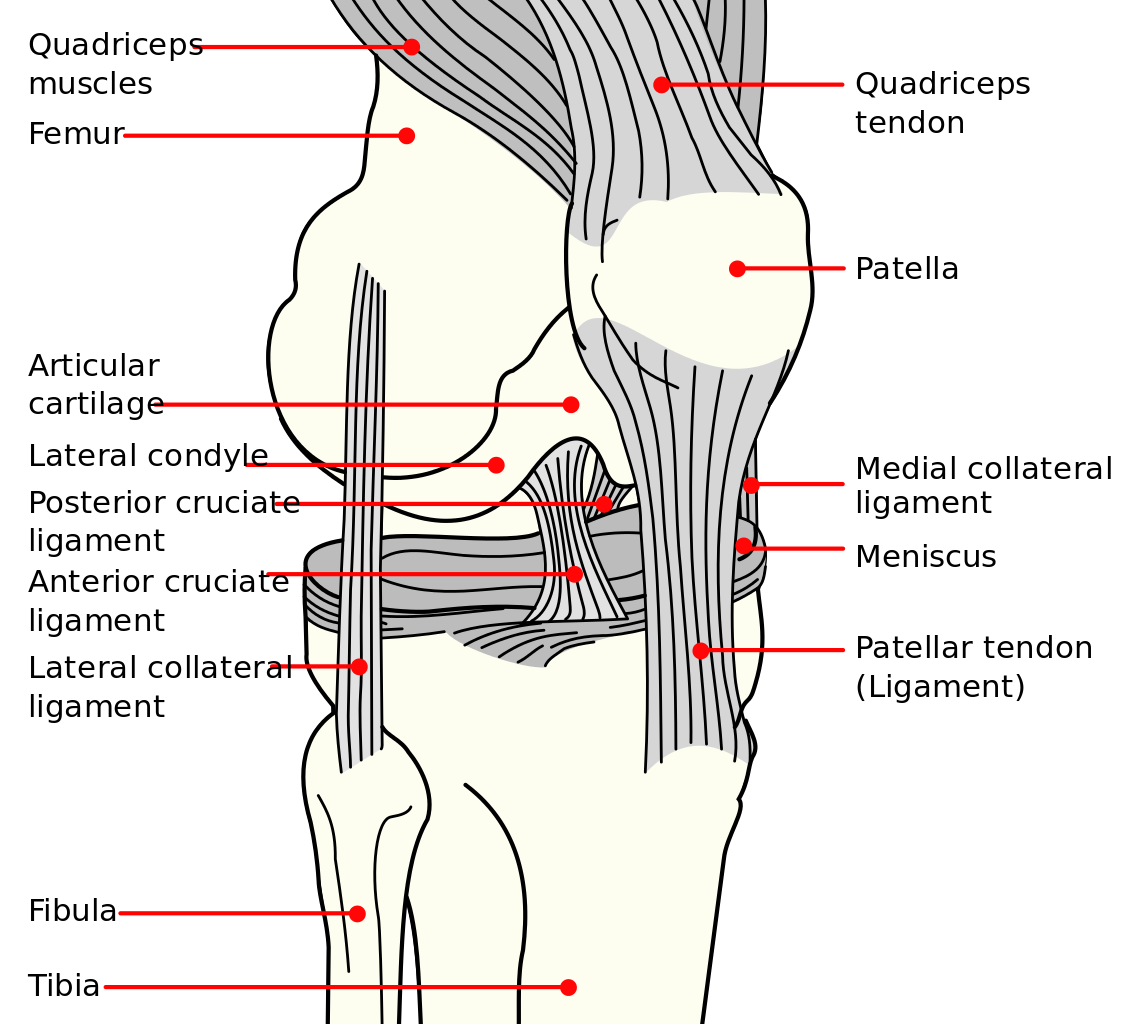
Front part of knee
Patellofemoral pain syndrome (anterior knee pain, variety of causations) Excessive medial drift of the knee during the power phase (very common)
Weak VMO (vastus medialis) and lateral knee structures
Seat set too low, can increase compression through the joint
Can involve medial or lateral retinaculum (kneecap ligaments) (all anterior knee pain can relate to the first two points)
Chondromalacia (damage to articular cartilage under the kneecap) A progression of above involving breakdown of the cartilage
Patellartendinosis (inflamed patella tendon) Excessive lateral traction of the kneecap
Quadriceps tendinosis (inflamed quadriceps tendon) Not very common but tends to affect the lateral aspect of the tendon
Outside Edge
Iliotibial band (ITB) friction syndrome
Excessive pressure on the ITB as it passes over the lateral femoral condyle. Can relate to incorrect bike set-up that increases the stretch on the ITB: saddle too high or too far back.
Leg length discrepancy: increased stretch on ITB in the shorter leg
Excessive tibial internal rotation that increases the pressure between the femoral condyle and the ITB. Can be anatomical or related to positioning of the cleat.
Inside Edge
Pes anserinus bursitis (inflamed bursa at hamstring tendinous insertion)
Excessive traction of the tendon over the bursa. Externally rotated tibial position, anatomical or related to cleat position.
Mediopatellar plica syndrome (inflamed thickened knee capsular fold)
Not very common, but can impinge on the femoral condyle during knee flexion
Back
Biceps femoris tendinosis (inflamed hamstring tendon insertion)
Saddle too high or too far back increases stretch on hamstrings. Excessive tibial internal rotation increases stretch on hamstrings0 -
Sometimes the knee pain, can stem from not having enough float in your cleats, and cleats not set in the best position on the shoes.
 0
0 -
sandbag wrote:Front part of knee
Patellofemoral pain syndrome (anterior knee pain, variety of causations) Excessive medial drift of the knee during the power phase (very common)
Weak VMO (vastus medialis) and lateral knee structures
Seat set too low, can increase compression through the joint
Can involve medial or lateral retinaculum (kneecap ligaments) (all anterior knee pain can relate to the first two points)
Chondromalacia (damage to articular cartilage under the kneecap) A progression of above involving breakdown of the cartilage
Patellartendinosis (inflamed patella tendon) Excessive lateral traction of the kneecap
Quadriceps tendinosis (inflamed quadriceps tendon) Not very common but tends to affect the lateral aspect of the tendon
Outside Edge
Iliotibial band (ITB) friction syndrome
Excessive pressure on the ITB as it passes over the lateral femoral condyle. Can relate to incorrect bike set-up that increases the stretch on the ITB: saddle too high or too far back.
Leg length discrepancy: increased stretch on ITB in the shorter leg
Excessive tibial internal rotation that increases the pressure between the femoral condyle and the ITB. Can be anatomical or related to positioning of the cleat.
Inside Edge
Pes anserinus bursitis (inflamed bursa at hamstring tendinous insertion)
Excessive traction of the tendon over the bursa. Externally rotated tibial position, anatomical or related to cleat position.
Mediopatellar plica syndrome (inflamed thickened knee capsular fold)
Not very common, but can impinge on the femoral condyle during knee flexion
Back
Biceps femoris tendinosis (inflamed hamstring tendon insertion)
Saddle too high or too far back increases stretch on hamstrings. Excessive tibial internal rotation increases stretch on hamstrings
Yep, and a friend of mine developed ITB and it was solved by lowering the seat and a slight adjustment of the cleat. The tendon on the outside of his knee was being stretched.0 -
sampras38 wrote:sandbag wrote:Front part of knee
Patellofemoral pain syndrome (anterior knee pain, variety of causations) Excessive medial drift of the knee during the power phase (very common)
Weak VMO (vastus medialis) and lateral knee structures
Seat set too low, can increase compression through the joint
Can involve medial or lateral retinaculum (kneecap ligaments) (all anterior knee pain can relate to the first two points)
Chondromalacia (damage to articular cartilage under the kneecap) A progression of above involving breakdown of the cartilage
Patellartendinosis (inflamed patella tendon) Excessive lateral traction of the kneecap
Quadriceps tendinosis (inflamed quadriceps tendon) Not very common but tends to affect the lateral aspect of the tendon
Outside Edge
Iliotibial band (ITB) friction syndrome
Excessive pressure on the ITB as it passes over the lateral femoral condyle. Can relate to incorrect bike set-up that increases the stretch on the ITB: saddle too high or too far back.
Leg length discrepancy: increased stretch on ITB in the shorter leg
Excessive tibial internal rotation that increases the pressure between the femoral condyle and the ITB. Can be anatomical or related to positioning of the cleat.
Inside Edge
Pes anserinus bursitis (inflamed bursa at hamstring tendinous insertion)
Excessive traction of the tendon over the bursa. Externally rotated tibial position, anatomical or related to cleat position.
Mediopatellar plica syndrome (inflamed thickened knee capsular fold)
Not very common, but can impinge on the femoral condyle during knee flexion
Back
Biceps femoris tendinosis (inflamed hamstring tendon insertion)
Saddle too high or too far back increases stretch on hamstrings. Excessive tibial internal rotation increases stretch on hamstrings
Yep, and a friend of mine developed ITB and it was solved by lowering the seat. The tendon on the outside of his knee was being stretched.
That as a solution can be a problem in itself because the longer leg then has problems. ITB problems should be sorted with stretching. Leg length descrepencies due to genetics, or through injury ie bones shorter on one leg, need a much more careful approach and that will usually involve shimming and adjusting shoes both in terms of height and fore/aft positioning in order that better symmetry can be achieved for the rider.0 -
doyler78 wrote:sampras38 wrote:sandbag wrote:Front part of knee
Patellofemoral pain syndrome (anterior knee pain, variety of causations) Excessive medial drift of the knee during the power phase (very common)
Weak VMO (vastus medialis) and lateral knee structures
Seat set too low, can increase compression through the joint
Can involve medial or lateral retinaculum (kneecap ligaments) (all anterior knee pain can relate to the first two points)
Chondromalacia (damage to articular cartilage under the kneecap) A progression of above involving breakdown of the cartilage
Patellartendinosis (inflamed patella tendon) Excessive lateral traction of the kneecap
Quadriceps tendinosis (inflamed quadriceps tendon) Not very common but tends to affect the lateral aspect of the tendon
Outside Edge
Iliotibial band (ITB) friction syndrome
Excessive pressure on the ITB as it passes over the lateral femoral condyle. Can relate to incorrect bike set-up that increases the stretch on the ITB: saddle too high or too far back.
Leg length discrepancy: increased stretch on ITB in the shorter leg
Excessive tibial internal rotation that increases the pressure between the femoral condyle and the ITB. Can be anatomical or related to positioning of the cleat.
Inside Edge
Pes anserinus bursitis (inflamed bursa at hamstring tendinous insertion)
Excessive traction of the tendon over the bursa. Externally rotated tibial position, anatomical or related to cleat position.
Mediopatellar plica syndrome (inflamed thickened knee capsular fold)
Not very common, but can impinge on the femoral condyle during knee flexion
Back
Biceps femoris tendinosis (inflamed hamstring tendon insertion)
Saddle too high or too far back increases stretch on hamstrings. Excessive tibial internal rotation increases stretch on hamstrings
Yep, and a friend of mine developed ITB and it was solved by lowering the seat. The tendon on the outside of his knee was being stretched.
That as a solution can be a problem in itself because the longer leg then has problems. ITB problems should be sorted with stretching. Leg length descrepencies due to genetics, or through injury ie bones shorter on one leg, need a much more careful approach and that will usually involve shimming and adjusting shoes both in terms of height and fore/aft positioning in order that better symmetry can be achieved for the rider.
Yep, agree with that completely and i think the guy in question had a very similar conversation with the guy that did the bike fitting, and they were looking at building up one of the cleats at one stage. I think that might have been the next step.0 -
My left calf seems to cramp up and not my right. Really unsure as to what is causing it. It seems to have happened since i built a single speed, so it must be a set-up issue. but I cant think what?0
-
birdy247 wrote:My left calf seems to cramp up and not my right. Really unsure as to what is causing it. It seems to have happened since i built a single speed, so it must be a set-up issue. but I cant think what?
Maybe a daft question but do you have 1 leg slightly longer than the other?
It might just be a cleat issue also and a good bike fit might help.0 -
I stuck my seat further forward today and beat my previous PB on a route by 1mph. Seat wont go any further forward but supposing if it's already set up high it's not an issue due to backward sloping seat tubes?
Well thanks for the thread anyway, it encouraged me to have a tinker with the set up") The British Empire never died, it just moved to the Velodrome0
The British Empire never died, it just moved to the Velodrome0 -
That's why plenty of experimentation with seat position is good. You can get it right and then start getting muscle imbalances. One way imbalance can be caused, If your style is to ride with feet, pointing inwards or outwards. Plenty of walking and other forms of weight leg exercise is good to do, to correct imbalances.
I find riding with the highest saddle position i can get away with, before the hips start rocking - is more efficient, but not good in the long term.0 -
Muscle Imbalances
Imbalances between the muscles on the outside (lateral quads, ITB) of the leg versus the inside (VMO): the lateral muscles can put a stronger pull on the kneecap than the VMO can meet, leading to weakness and strain of the VMO. The VMO is particularly susceptible to weakening after knee injury where the leg is immobilised or full range of knee motion is restricted for a period of time. Sometimes clients will report a feeling of strain or tenderness just to the top inside of the knee which they can feel by pressing when the knee is bent. They notice it during cycling, running or stair climbing. This can be a sign that the VMO is weak, and if not addressed could later lead to pain around the kneecap.
Studies have shown that tight ITB, weak gluteus medius and abductors, weak external rotators, and weak core can give rise to instability in the pelvis. Pelvic instability can cause the thigh bone (femur) to rotate inward more than usual. This might be observed as a side to side movement of the knee when extending the leg during the downstroke, instead of the desired linear movement of the knee as you push down on the pedal. This changes the orientation of the groove so the kneecap does not track in it properly leading to pain. A rough test of your pelvic stability would be to perform a lunge or squat and note whether the knee rolls inwards as you perform it. Your knee should keep pointing straight and not dip or turn inwards. Or alternatively as mentioned in the article on ITB problems, excessive hip dipping while cycling would also be another indicator that the gluteus medius and abductor s are weak.
Anatomical Reasons
Increased foot pronation. Pronation is the rolling inwards of the foot during walking or running or cycling. Excessive pronation or over pronation can lead to problems at the knee. While this movement happens at the foot, it also causes a compensatory movement in the shin bone which affects the alignment at the knee impacting the kneecap and causing pain.
The position of the shin bone, excessive inward or outward rotation of the lower leg can affect the alignment at the knee. It has been suggested that people with low arches may be more susceptible to PFP than those with normal arches as low arches change the alignment of the shin bone. The positioning of your cleats can affect the position of the shin bone and the rotation of the lower leg.
Leg length discrepancies: when setting saddle height only one leg is correctly fitted to the pedal meaning that if the bike is fitted to suit the shorter leg, there will be increased compression of the kneecap in the groove and pain. Leg length discrepancies can occur due to rotations at the pelvis, or more unusually, if you were born with them.Exercises
Neuromuscular control of VMO
This exercise ensures that the VMO is contracting correctly. This ability to contract correctly and at the right time (called neuromuscular control) can be inhibited by pain or swelling in the knee. Sit on the ground with your leg outstretched in front of you. Put your hand just above the knee and a little to the inside – this is the VMO. Now try and bring the back of your knee to touch the floor, i.e. straighten the leg more. You should feel your VMO contract. If not repeat this exercise until you can feel the VMO start to contract, and continue it until the VMO is contracting for each repetition. Progress to trying this standing up when weight bearing on the leg so the exercise then becomes more functional.
VMO Alphabet
Once the VMO is contracting properly, this exercise will help to continue strengthen it.
Sit on the floor and support your body weight on your hands
Raise your leg approx 6 inches (15 cm) off the floor.
Keeping your leg straight, point you foot and using your foot as a “pen” draw the alphabet in the air.
The movements should be small and you should feel the VMO working as you do the exercise.
Strengthening the gluteus medius.
See the article on the ITB pain for pictures of the exercise.
Lie on your side with the side to be strengthened on top
Bend the lower leg slightly at the hip and knee for stability
Bring the leg backwards so it lies behind the hip.
Slowly raise the upper leg until 1-2 inches over the hip
From this position slowly lower the leg (1 repetition)
Repeat: 10-12 repetitions on each side, and build up to being able to perform 3 sets, three times a week
Note: place your hand on the gluteus medius – this is located above and to the outside of your jeans back pockets. You should feel the contraction here as you raise your leg upwards. It is important to keep the leg behind you as this localises the effort to the gluteus medius muscle, if it comes forward to much other muscles become involved. Also do not raise the leg much over the level of hip, raising it higher just involves use of the back muscles and it’s not working the gluteus medius. Add ankle weights if 3 sets can be done easily.
Lunges or squats
When you have built up the strength of the VMO and gluteus medius perform a lunge or squat exercise. With weak pelvic stablisers, the knee can roll inwards when performing a squat or lunge. The aim of this exercise is to develop knee control and to further strengthen the quads, abductors and gluteal muscles so that the knee does not roll inward. When performing the exercise the ensure knee stays in line with the toes and does not move inwards over the side of the foot. Use a wall or stable surface for balance to help you get the movement right and under control. Make sure to stretch quads after these exercises. Repetitions: 10-12. No of Sets: 3, three times a week.
Karen is a Physical Therapist and member of the Irish Association of Physical Therapists. She worked on the Rás in 2008 with the Dundrum Orwell team, and in 2009 with the Irish National Team, and more recently accompanied the National Junior and U23 track team to the European Championships in 2009.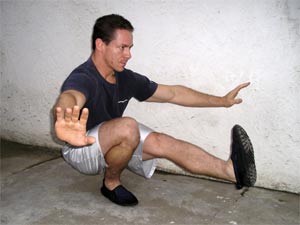 0
0 -
just to comment on this i am recovering from a soft tissue injury to the left knee and when i reviewed my bike set up i found that the seat was too high by about 1cm and about 1cm too far forward0
-
Steve Hogg even mentions this.0
-
How did you find this?paul.k wrote:just to comment on this i am recovering from a soft tissue injury to the left knee and when i reviewed my bike set up i found that the seat was too high by about 1cm and about 1cm too far forwardCAPTAIN BUCKFAST'S CYCLING TIPS - GUARANTEED TO WORK! 1 OUT OF 10 RACING CYCLISTS AGREE!0 -
hopefully, this still realtes to the OP topic: what part of the seat should you be sitting on since moving forwards/backwards on the seat gives very different positions. I ask because I was watching Cadel Evans on the Giro and he seemed to have several inches of seat visible behind his backside whilst riding.0
-
You may find this interesting too..........http://bikedynamics.co.uk/FitGuideTT.htm...................................................................................................
If you want to be a strong rider you have to do strong things.
However if you train like a cart horse you'll race like one.0